INTERMEZZO
-
zolpidem tartrate tablet
Purdue Pharma LP
----------
| HIGHLIGHTS OF PRESCRIBING INFORMATION | These highlights do not include all the information needed to use INTERMEZZO® safely and effectively. See full prescribing information for INTERMEZZO.
INTERMEZZO® (zolpidem tartrate) sublingual tablets, CIV
Initial U.S. Approval: 1992
| INDICATIONS AND USAGE | Intermezzo is a GABAA agonist indicated for use as needed for the treatment of insomnia when a middle-of-the-night awakening is followed by difficulty returning to sleep (1) Limitation of Use: Not indicated for the treatment of middle-of-the night awakening when the patient has fewer than 4 hours of bedtime remaining before the planned time of waking (1)
| DOSAGE AND ADMINISTRATION | - Take only if 4 hours of bedtime remain before the planned time of waking (2.1, 5.1)
- Intermezzo should be placed under the tongue and allowed to disintegrate completely before swallowing. The tablet should not be swallowed whole. (2.1)
- The effect of Intermezzo may be slowed if taken with or immediately after a meal (2.1)
- Recommended dose is 1.75 mg for women and 3.5 mg for men, taken only once per night if needed (2.2)
- Lower doses of CNS depressants may be necessary when taken concomitantly with Intermezzo (2.3)
- Co-administration with CNS depressants: Recommended dose is 1.75 mg for men and women (2.3)
- Geriatric patients and patients with hepatic impairment: Recommended dose is 1.75 mg for men and women (2.4, 2.5)
| DOSAGE FORMS AND STRENGTHS | 1.75 mg and 3.5 mg sublingual tablets (3)
| CONTRAINDICATIONS | Known hypersensitivity to zolpidem (4)
| WARNINGS AND PRECAUTIONS | - CNS depressant effects: Impairs alertness and motor coordination. Instruct patients on correct use (5.1)
- Evaluate for co-morbid diagnoses: Re-evaluate if insomnia persists after 7 to 10 days of use (5.2)
- Severe anaphylactic/anaphylactoid reactions: Angioedema and anaphylaxis have been reported. Do not re-challenge if such reactions occur (5.3)
- “Sleep-driving” and other complex behaviors while not fully awake. Risk increases with dose and use with other CNS depressants and alcohol. Immediately evaluate any new onset behavioral changes (5.4)
- Depression: Worsening of depression or suicidal thinking may occur. Prescribe the least number of tablets feasible to avoid intentional overdose (5.5)
- Respiratory Depression: Consider this risk before prescribing in patients with compromised respiratory function (5.6)
| ADVERSE REACTIONS | Most commonly observed adverse reactions (> 1% in adult patients) are headache, nausea, and fatigue. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Purdue Pharma at 1-888-726-7535 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
| DRUG INTERACTIONS | - CNS depressants, including alcohol: Possible adverse additive CNS depressant effects (5.1, 7.1)
- Imipramine: Decreased alertness observed (7.1)
- Chlorpromazine: Impaired alertness and psychomotor performance observed (7.1)
- Rifampin: Combination use may decrease effects (7.2)
- Ketoconazole: Combination use may increase effects (7.2)
| USE IN SPECIFIC POPULATIONS | - Pregnancy: Based on animal data, zolpidem may cause fetal harm. (8.1)
- Pediatric use: Safety and effectiveness of Intermezzo not established. With bedtime dosing of zolpidem, hallucinations observed (incidence 7%) (8.4)
|
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide |
Revised: 07/2015 |
|
FULL PRESCRIBING INFORMATION1 INDICATIONS AND USAGE
Intermezzo® (zolpidem tartrate) sublingual tablet is indicated for use as needed for the treatment of insomnia when a middle-of-the-night awakening is followed by difficulty returning to sleep.
Limitations of Use: Intermezzo is not indicated for the treatment of middle-of-the-night insomnia when the patient has fewer than 4 hours of bedtime remaining before the planned time of waking.
2 DOSAGE AND ADMINISTRATION
2.1 Important Administration Instructions
Intermezzo is to be taken in bed when a patient wakes in the middle of the night and has difficulty returning to sleep. Intermezzo should only be taken if the patient has at least 4 hours of bedtime remaining before the planned time of waking [see Warnings and Precautions (5.1)].
Intermezzo should be placed under the tongue and allowed to disintegrate completely before swallowing. The tablet should not be swallowed whole. For optimal effect, Intermezzo should not be administered with or immediately after a meal. The tablet should be removed from the pouch just prior to dosing.
2.2 Basic Dosing Information
The recommended and maximum dose of Intermezzo is 1.75 mg for women and 3.5 mg for men, taken only once per night as needed if a middle-of-the-night awakening is followed by difficulty returning to sleep. The recommended doses for women and men are different because women clear zolpidem from the body at a lower rate than men[see Use in Specific Populations (8.6)].
2.3 Use with CNS Depressants
The recommended Intermezzo dose for men and women who are taking concomitant CNS depressants is 1.75 mg. Dose adjustment of concomitant CNS depressants may be necessary when co-administered with Intermezzo because of potentially additive effects. The use of Intermezzo with other sedative-hypnotics (including other zolpidem products) at bedtime or the middle of the night is not recommended [see Warnings and Precautions (5.1)].
2.4 Use in Geriatric Patients
Geriatric patients may be especially sensitive to the effects of zolpidem. The recommended dose of Intermezzo in men and women over 65 years old is 1.75 mg, taken only once per night if needed [see Use in Specific Populations (8.5)].
2.5 Use in Patients with Hepatic Impairment
The recommended dose of Intermezzo in patients with hepatic impairment is 1.75 mg, taken only once per night if needed [see Clinical Pharmacology (12.3)].
3 DOSAGE FORMS AND STRENGTHS
Intermezzo is available as 1.75 mg and 3.5 mg tablets for sublingual administration.
Intermezzo 1.75 mg tablets are yellow, round, uncoated, biconvex, debossed with ZZ on one side.
Intermezzo 3.5 mg tablets are beige, round, uncoated, biconvex, debossed with ZZ on one side.
4 CONTRAINDICATIONS
Intermezzo is contraindicated in patients with known hypersensitivity to zolpidem. Observed reactions with zolpidem include anaphylaxis and angioedema [see Warnings and Precautions (5.3)].
5 WARNINGS AND PRECAUTIONS
5.1 CNS Depressant Effects and Next-Day Impairment
Intermezzo, like other sedative-hypnotic drugs, has central nervous system (CNS) depressant effects. Co-administration with other CNS depressants (e.g., benzodiazepines, opioids, tricyclic antidepressants, alcohol) increases the risk of CNS depression. Dosage adjustments of Intermezzo and of other concomitant CNS depressants may be necessary when Intermezzo is administered with such agents because of the potentially additive effects. The use of Intermezzo with other sedative-hypnotics (including other zolpidem products) at bedtime or the middle of the night is not recommended [see Dosage and Administration (2.3)].
In a driving study, healthy subjects who received Intermezzo with fewer than four hours of bedtime remaining had evidence of impaired driving compared to subjects who received placebo [see Clinical Studies (14.2)]. The risk of next-day driving impairment (and psychomotor impairment) is increased if Intermezzo is taken with less than 4 hours of bedtime remaining, if higher than recommended dose is taken, if co-administered with other CNS depressants, or co-administered with other drugs that increase the blood levels of zolpidem.
5.2 Need to Evaluate for Co-morbid Diagnoses
Because sleep disturbances may be the presenting manifestation of a physical and/or psychiatric disorder, symptomatic treatment of insomnia should be initiated only after a careful evaluation of the patient. The failure of insomnia to remit after 7 to 10 days of treatment may indicate the presence of a primary psychiatric and/or medical illness that should be evaluated. Worsening of insomnia or the emergence of new thinking or behavior abnormalities may be the consequence of an unrecognized psychiatric or physical disorder. Such findings have emerged during the course of treatment with sedative-hypnotic drugs, including zolpidem.
5.3 Severe Anaphylactic and Anaphylactoid Reactions
Cases of angioedema involving the tongue, glottis, or larynx have been reported in patients after taking the first or subsequent doses of zolpidem. Some patients have had additional symptoms such as dyspnea, throat closing, or nausea and vomiting that suggest anaphylaxis. Some patients have required medical therapy in the emergency department. If angioedema involves the throat, glottis or larynx, airway obstruction may occur and be fatal. Patients who develop angioedema or anaphylaxis after treatment with zolpidem should not be rechallenged with Intermezzo.
5.4 Abnormal Thinking and Behavioral Changes
Abnormal thinking and behavior changes have been reported in patients treated with sedative-hypnotics including zolpidem. Some of these changes included decreased inhibition (e.g., aggressiveness and extroversion that seemed out of character), bizarre behavior, agitation, and depersonalization. Visual and auditory hallucinations have also been reported.
In controlled trials of zolpidem tartrate 10 mg taken at bedtime, < 1% of adults with insomnia who received zolpidem reported hallucinations. In a clinical trial, 7% of pediatric patients treated with zolpidem tartrate 0.25 mg/kg taken at bedtime, reported hallucinations, versus 0% treated with placebo [see Use in Specific Populations (8.4)].
Complex behaviors such as “sleep-driving” (i.e., driving while not fully awake after ingestion of a sedative-hypnotic, with amnesia for the event) have been reported in sedative-hypnotic-naive as well as in sedative-hypnotic-experienced persons. Although behaviors such as “sleep-driving” have occurred with zolpidem alone at therapeutic doses, the co-administration of zolpidem with alcohol and other CNS depressants increases the risk of such behaviors, as does the use of zolpidem at doses exceeding the maximum recommended dose. Due to the risk to the patient and the community, discontinuation of Intermezzo should be strongly considered for patients who report a “sleep-driving” episode.
Other complex behaviors (e.g., preparing and eating food, making phone calls, or having sex) have been reported in patients who are not fully awake after taking a sedative-hypnotic. As with “sleep-driving”, patients usually do not remember these events. Amnesia, anxiety and other neuro-psychiatric symptoms may also occur.
The emergence of any new behavioral sign or symptom of concern requires careful and immediate evaluation.
5.5 Use in Patients with Depression
In primarily depressed patients treated with sedative-hypnotics, worsening of depression, and suicidal thoughts and actions (including completed suicides), have been reported. Suicidal tendencies may be present in such patients and protective measures may be required. Intentional overdosage is more common in this group of patients; therefore, the lowest number of tablets that is feasible should be prescribed for the patient at any one time.
5.6 Respiratory Depression
Although studies with 10 mg zolpidem tartrate did not reveal respiratory depressant effects at hypnotic doses in healthy subjects or in patients with mild-to-moderate chronic obstructive pulmonary disease (COPD), a reduction in the Total Arousal Index, together with a reduction in lowest oxygen saturation and increase in the times of oxygen desaturation below 80% and 90%, was observed in patients with mild-to-moderate sleep apnea when treated with zolpidem compared to placebo. Since sedative-hypnotics have the capacity to depress respiratory drive, precautions should be taken if Intermezzo is prescribed to patients with compromised respiratory function. Post-marketing reports of respiratory insufficiency in patients receiving 10 mg of zolpidem tartrate, most of whom had pre-existing respiratory impairment, have been reported. The risks of respiratory depression should be considered prior to prescribing Intermezzo in patients with respiratory impairment including sleep apnea and myasthenia gravis.
5.7 Withdrawal Effects
There have been reports of withdrawal signs and symptoms following the rapid dose decrease or abrupt discontinuation of zolpidem. Monitor patients for tolerance, abuse, and dependence [see Drug Abuse and Dependence (9.2) and (9.3)].
6 ADVERSE REACTIONS
The following serious adverse reactions in zolpidem-treated patients are discussed in greater detail in other sections of the labeling:
- CNS-depressant effects and next-day impairment [see Warnings and Precautions (5.1)]
- Serious anaphylactic and anaphylactoid reactions [see Warnings and Precautions (5.3)]
- Abnormal thinking and behavioral changes, and complex behaviors [see Warnings and Precautions (5.4)]
- Withdrawal effects [see Warnings and Precautions (5.7)]
6.1 Clinical Trials Experience
The safety data described below are based on two double-blind placebo-controlled trials of Intermezzo in adult patients with insomnia characterized by difficulty returning to sleep after a middle-of-the-night awakening [see Clinical Studies (14.1)]. These two trials included 230 and 82 patients treated with 3.5 mg and 1.75 mg of Intermezzo, respectively. The first study was a 3-way crossover sleep-laboratory study in 82 patients (58 female and 24 male; median age 47 years; 51% Caucasian, 44% African-American) of 1.75 mg and 3.5 mg of Intermezzo compared to placebo (Study 1). The second study was a 4-week, parallel-group at-home study in 295 patients (201 female and 94 male; median age 43 years) of 3.5 mg of Intermezzo compared to placebo, used on an as-needed basis after spontaneous middle-of-the-night awakenings (Study 2). In Study 2, patients took Intermezzo during the night on 62% of study nights.
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in actual practice.
Table 1 shows the incidence of adverse reactions reported in Study 2 that occurred in 2% or more of Intermezzo-treated (3.5 mg) patients in which the incidence was greater than the incidence in placebo-treated patients. For women and other patients taking the 1.75 mg dose in Study 1, the incidence of adverse reactions was similar to the incidence seen with 3.5 mg of Intermezzo in Table 1.
The most commonly reported adverse reactions in all treatment groups were headache, nausea, and fatigue.
Table 1: Summary of Adverse Reactions (≥ 2%) in Outpatient, Double-Blind, Parallel-Group, Placebo-Controlled Study (Study 2)| MedDRA System Organ Class Preferred Term | 3.5 mg Intermezzo
(n=150) | Placebo
(n=145) |
|---|
| Gastrointestinal Disorders | 4% | 2% |
| Nausea | 1% | 1% |
| General Disorders and Administration Site Conditions | 3% | 0% |
| Fatigue | 1% | 0% |
| Nervous System Disorders | 5% | 3% |
| Headache | 3% | 1% |
6.2 Post Marketing Experience
The following adverse reactions, have been identified during post-approval use of intermezzo. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to establish a causal relationship to drug exposure.
- Application site reactions primarily in the subligual area, have been reported. These application site reactions included oral ulcers, blisters, and mucosal inflammation.
7 DRUG INTERACTIONS
7.1 CNS-active Drugs
Co-administration of zolpidem with other CNS depressants increases the risk of CNS depression [see Warnings and Precautions (5.1)]. Zolpidem tartrate was evaluated in healthy volunteers in single-dose interaction studies for several CNS drugs.
Imipramine
Imipramine in combination with zolpidem produced no pharmacokinetic interaction other than a 20% decrease in peak levels of imipramine, but there was an additive effect of decreased alertness. Similarly, chlorpromazine in combination with zolpidem produced no pharmacokinetic interaction, but there was an additive effect of decreased alertness and psychomotor performance.
Haloperidol
A study involving haloperidol and zolpidem revealed no effect of haloperidol on the pharmacokinetics or pharmacodynamics of zolpidem. The lack of a drug interaction following single-dose administration does not predict the absence of an effect following chronic administration.
Alcohol
An additive adverse effect on psychomotor performance between alcohol and oral zolpidem was demonstrated [see Warnings and Precautions (5.1)].
Sertraline
Concomitant administration of zolpidem and sertraline increases exposure to zolpidem and may increase the pharmacodynamic effect of zolpidem.
Fluoxetine
After multiple doses of zolpidem tartrate and fluoxetine, an increase in the zolpidem half-life (17%) was observed. There was no evidence of an additive effect in psychomotor performance [see Clinical Pharmacology (12.3)].
7.2 Drugs that Affect Drug Metabolism via Cytochrome P450
Some compounds known to inhibit CYP3A may increase exposure to zolpidem. The effect of other P450 enzymes on the exposure to zolpidem is not known.
Rifampin
Rifampin, a CYP3A4 inducer, significantly reduced the exposure to and the pharmacodynamic effects of zolpidem. Use of rifampin in combination with zolpidem may decrease the efficacy of zolpidem.
Ketoconazole
Ketoconazole, a potent CYP3A4 inhibitor, increased the pharmacodynamic effects of zolpidem. Consideration should be given to using a lower dose of zolpidem when ketoconazole and zolpidem are given together.
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Category C
There are no adequate and well-controlled studies of zolpidem in pregnant women. Studies in children to assess the effects of prenatal exposure to zolpidem have not been conducted; however, cases of severe neonatal respiratory depression have been reported when zolpidem was used at the end of pregnancy, especially when taken with other CNS-depressants. Children born to mothers taking sedative-hypnotic drugs may be at risk for withdrawal symptoms during the postnatal period. Neonatal flaccidity has also been reported in infants born to mothers who received sedative-hypnotic drugs during pregnancy. Intermezzo should be used during pregnancy only if the potential benefit outweighs the potential risk to the fetus.
Administration of zolpidem to pregnant rats and rabbits resulted in adverse effects on offspring at doses greater than the recommended human dose (RHD) of 3.5 mg/day (approximately 2.8 mg/day zolpidem base); however, teratogenicity was not observed.
When zolpidem was administered at oral doses of 4, 20, and 100 mg base/kg/day to pregnant rats during the period of organogenesis, dose-related decreases in fetal skull ossification were observed at all but the lowest dose, which is approximately 15 times the RHD on a mg/m2 basis. In rabbits treated during organogenesis with zolpidem at oral doses of 1, 4, and 16 mg base/kg/day, increased embryo-fetal death and incomplete fetal skull ossification were seen at the highest dose tested. The no-effect dose for embryo-fetal toxicity in rabbits is approximately 30 times the RHD on a mg/m2 basis. Administration of zolpidem to rats at oral doses of 4, 20, and 100 mg base/kg/day during the latter part of pregnancy and throughout lactation produced decreased offspring growth and survival at all but the lowest dose, which is approximately 15 times the RHD on a mg/m2 basis.
8.3 Nursing Mothers
Zolpidem is excreted in human milk. The effect of zolpidem on the nursing infant is not known.
8.4 Pediatric Use
Intermezzo is not recommended for use in children. Safety and effectiveness of Intermezzo have not been established in pediatric patients below the age of 18.
In an 8-week study in pediatric patients (aged 6 to 17 years) with insomnia associated with ADHD, an oral solution of zolpidem tartrate dosed at 0.25 mg/kg at bedtime did not decrease sleep latency compared to placebo. Hallucinations were reported in 7% of the pediatric patients who received zolpidem; none of the pediatric patients who received placebo reported hallucinations.
8.5 Geriatric Use
Intermezzo dosage adjustment is necessary in geriatric patients. Sedating drugs may cause confusion and over-sedation in the elderly; elderly patients generally should be started on low doses of Intermezzo and observed closely [see Dosage and Administration (2.4), and Clinical Pharmacology (12.3)].
Clinical trial experience with other zolpidem formulations (5 mg to 10 mg oral zolpidem tartrate) given at bedtime:
A total of 154 patients in U.S.-controlled clinical trials and 897 patients in non-U.S. clinical trials who received oral zolpidem were ≥ 60 years of age. For a pool of U.S. patients receiving oral zolpidem tartrate at doses of ≤ 10 mg or placebo, there were three adverse reactions occurring at an incidence of at least 3% for zolpidem and for which the zolpidem incidence was at least twice the placebo incidence (see Table 2).
Table 2: Adverse Reactions in Geriatric Patients in Pooled Trials of 5 mg to 10 mg of Oral Zolpidem Tartrate Given at Bedtime| Adverse Reaction | 5 to 10 mg Oral
Zolpidem tartrate | Placebo |
| Dizziness | 3% | 0% |
| Drowsiness | 5% | 2% |
| Diarrhea | 3% | 1% |
Falls in geriatric patients:
A total of 30/1,959 (2%) non-U.S. patients receiving other zolpidem formulations (5 mg to 10 mg oral zolpidem tartrate) reported falls, including 28/30 (93%) who were ≥ 70 years of age. Of these 28 patients, 23 (82%) were receiving zolpidem tartrate doses > 10 mg. A total of 24/1,959 (1%) non-U.S. patients receiving zolpidem reported confusion, including 18/24 (75%) who were ≥70 years of age. Of these 18 patients, 14 (78%) were receiving zolpidem tartrate doses >10 mg.
The dose of Intermezzo in elderly patients is 1.75 mg to minimize adverse effects related to impaired motor and/or cognitive performance and unusual sensitivity to sedative-hypnotic drugs.
8.6 Gender Difference in Pharmacokinetics
Women cleared zolpidem tartrate from the body after sublingual administration of a 3.5 mg dose of Intermezzo at a lower rate than men (2.7 mL/min/kg vs. 4.0 mL/min/kg). Cmax and AUC parameters of zolpidem were approximately 45% higher at the same dose in female subjects compared with male subjects. Given the higher blood levels of zolpidem tartrate in women compared to men at a given dose, the recommended dose of Intermezzo for women is 1.75 mg, and the recommended dose for adult men is 3.5 mg.
9 DRUG ABUSE AND DEPENDENCE
9.1 Controlled Substance
Zolpidem tartrate is classified as a Schedule IV controlled substance by federal regulation.
9.2 Abuse
Abuse and addiction are separate and distinct from physical dependence and tolerance. Abuse is characterized by misuse of the drug for non-medical purposes, often in combination with other psychoactive substances. Tolerance is a state of adaptation in which exposure to a drug induces changes that result in diminution of one or more of the drug effects over time. Tolerance may occur to both desired and undesired effects of drugs and may develop at different rates for different effects.
Addiction is a primary, chronic, neurobiological disease with genetic, psychosocial, and environmental factors influencing its development and manifestations. It is characterized by behaviors that include one or more of the following: impaired control over drug use, compulsive use, continued use despite harm, and craving. Drug addiction is a treatable disease, using a multidisciplinary approach, but relapse is common.
Studies of abuse potential in former drug abusers found that the effects of single doses of 40 mg of oral zolpidem tartrate were similar, but not identical, to diazepam 20 mg, while 10 mg of oral zolpidem tartrate was difficult to distinguish from placebo.
Because persons with a history of addiction to or abuse of drugs or alcohol are at increased risk for misuse, abuse and addiction of zolpidem, they should be monitored carefully when receiving Intermezzo.
9.3 Dependence
Physical dependence is a state of adaptation that is manifested by a specific withdrawal syndrome that can be produced by abrupt cessation, rapid dose reduction, decreasing blood level of the drug, and/or administration of an antagonist.
Sedative-hypnotics have produced withdrawal signs and symptoms following abrupt discontinuation. These reported symptoms range from mild dysphoria and insomnia to a withdrawal syndrome that may include abdominal and muscle cramps, vomiting, sweating, tremors, and convulsions. The following adverse events which are considered to meet the DSM-III-R criteria for uncomplicated sedative-hypnotic withdrawal were reported during U.S. clinical trials with other oral zolpidem formulations following placebo substitution occurring within 48 hours following the last zolpidem treatment: fatigue, nausea, flushing, lightheadedness, uncontrolled crying, emesis, stomach cramps, panic attack, nervousness, and abdominal discomfort. These reported adverse events occurred at an incidence of 1% or less. However, available data cannot provide a reliable estimate of the incidence, if any, of dependence during treatment at recommended doses. Post-marketing reports of abuse, dependence, and withdrawal resulting from use of oral zolpidem tartrate have been received.
10 OVERDOSAGE
10.1 Signs and Symptoms
In post-marketing experience of overdose with oral zolpidem tartrate alone, or in combination with CNS-depressant agents, impairment of consciousness ranging from somnolence to coma, cardiovascular and/or respiratory compromise, and fatal outcomes have been reported.
10.2 Recommended Treatment
General symptomatic and supportive measures should be used along with immediate gastric lavage where appropriate. Intravenous fluids should be administered as needed. Zolpidem’s sedative-hypnotic effect was shown to be reduced by flumazenil and therefore flumazenil may be useful; however, flumazenil administration may contribute to the appearance of neurological symptoms (convulsions). As in all cases of drug overdose, respiration, pulse, blood pressure, and other appropriate signs should be monitored and general supportive measures employed. Hypotension and CNS depression should be treated by appropriate medical intervention. Sedating drugs should be withheld following zolpidem overdosage, even if excitation occurs. The value of dialysis in the treatment of overdosage has not been determined, although hemodialysis studies in patients with renal failure receiving therapeutic doses have demonstrated that zolpidem is not dialyzable.
As with management of all overdosage, the possibility of multiple drug ingestion should be considered. The healthcare provider may wish to consider contacting a poison control center for up-to-date information on the management of hypnotic drug overdosage.
11 DESCRIPTION
Intermezzo contains zolpidem tartrate, a non-benzodiazepine hypnotic of the imidazopyridine class. Intermezzo is available in 1.75 mg and 3.5 mg strength tablets for sublingual administration. Intermezzo sublingual tablets are intended to be placed under the tongue where they will disintegrate.
Intermezzo sublingual tablets contain a bicarbonate-carbonate buffer.
Chemically, zolpidem tartrate is N,N-6-trimethyl-2-p-tolylimidazo[1,2-α]pyridine-3-acetamide L-(+)-tartrate (2:1).
Zolpidem tartrate is a white to off-white crystalline powder that is sparingly soluble in water, alcohol, and propylene glycol. It has a molecular weight of 764.88.
Each Intermezzo tablet includes the following inactive ingredients: mannitol, sorbitol, crospovidone, silicon dioxide, sodium carbonate, sodium bicarbonate, croscarmellose sodium, sodium stearyl fumarate, silicon dioxide, natural and artificial spearmint flavor, silicon dioxide-colloidal, and sucralose. The 1.75 mg tablet also contains yellow iron oxide, and the 3.5 mg tablet contains beige iron oxide.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Zolpidem, the active moiety of zolpidem tartrate, is a hypnotic agent with a chemical structure unrelated to benzodiazepines, barbiturates, or other drugs with known hypnotic properties. It interacts with a GABA-BZ complex and shares some of the pharmacological properties of the benzodiazepines. In contrast to the benzodiazepines, which nonselectively bind to and activate all BZ receptor subtypes, zolpidem in vitro binds the BZ1 receptor preferentially with a high affinity ratio of the alpha1/alpha5 subunits. This selective binding of zolpidem on the BZ1 receptor is not absolute, but it may explain the relative absence of myorelaxant and anticonvulsant effects in animal studies as well as the preservation of deep sleep (stages 3 and 4) in human studies of zolpidem at hypnotic doses.
12.3 Pharmacokinetics
Absorption
Intermezzo disintegrates in the sublingual cavity after administration. On average, Intermezzo is rapidly absorbed in both genders, with a mean Tmax across studies of about 35 minutes to about 75 minutes.
In healthy normal volunteers (age 21 to 45 years) dosed with 3.5 mg Intermezzo, the average Cmax and AUC were 77 ng/mL and 296 ng•h/mL, respectively in women. The average Cmax and AUC were 53 ng/mL and 198 ng•h/mL, respectively in men. In women, the average Cmax and AUC of the 1.75 mg Intermezzo dose were 37 ng/mL and 151 ng•h/mL, respectively.
Food decreased the overall Cmax and AUC of Intermezzo 3.5 mg by 42% and 19%, respectively, and increased the time to peak exposure (Tmax) to nearly 3 hours. For optimal effect, Intermezzo should not be administered with or immediately after a meal.
Distribution
Based on data obtained with oral zolpidem, the total protein binding was found to be 93% ± 0.1% and remained constant independent of concentration between 40 ng/mL and 790 ng/mL.
Metabolism
Based on data obtained with oral zolpidem, zolpidem tartrate is converted to inactive metabolites that are eliminated primarily by renal excretion.
Elimination
The elimination half-life of a single dose of a 3.5 mg Intermezzo sublingual tablet is approximately 2.5 hours (range 1.4 to 3.6 hours).
Special Populations
Elderly: The recommended dose for Intermezzo is 1.75 mg. A pharmacokinetic study of 1.75 mg and 3.5 mg doses of Intermezzo showed that the plasma Cmax and AUC0-4 hr in elderly subjects following the 3.5 mg dose was higher by 34% and 30%, respectively, than the non-elderly subjects. The Cmax and AUC of 1.75 mg in elderly subjects were consistently lower than those observed for the 3.5 mg dose in non-elderly subjects but consistently higher than the 1.75 mg dose in non-elderly subjects. The elimination half-life remained unchanged.
Hepatic Impairment: The pharmacokinetics of oral zolpidem tartrate in eight patients with chronic hepatic insufficiency were compared to results in subjects with normal hepatic function. Following a single 20 mg oral zolpidem tartrate dose, mean Cmax and AUC were found to be two times (250 ng/mL vs. 499 ng/mL) and five times (788 ng•hr/mL vs. 4203 ng•hr/mL) higher, respectively, in hepatically compromised patients compared to subjects with normal hepatic function. Tmax did not change. The mean half-life in cirrhotic patients of 9.9 hr (range: 4.1 to 25.8 hr) was greater than that observed in subjects with normal hepatic function of 2.2 hr (range: 1.6 to 2.4 hr). Dosing should be modified accordingly in patients with hepatic insufficiency [see Dosage and Administration (2.5)].
Renal Impairment: The pharmacokinetics of zolpidem tartrate were studied in 11 patients with end-stage renal failure (mean ClCr= 6.5 ± 1.5 mL/min) undergoing hemodialysis three times a week, who were dosed with zolpidem tartrate 10 mg orally each day for 14 or 21 days. No statistically significant differences were observed for Cmax, Tmax, half-life, and AUC between the first and last day of drug administration when baseline concentration adjustments were made. Zolpidem was not hemodialyzable. No accumulation of unchanged drug appeared after 14 or 21 days. Zolpidem pharmacokinetics were not significantly different in renally-impaired patients. No dosage adjustment is necessary in patients with renal impairment.
Drug Interactions
CNS-depressants
Co-administration of zolpidem with other CNS depressants increases the risk of CNS depression [see Warnings and Precautions (5.1)]. Zolpidem tartrate was evaluated in healthy volunteers in single-dose interaction studies for several CNS drugs. Imipramine in combination with zolpidem produced no pharmacokinetic interaction other than a 20% decrease in peak levels of imipramine, but there was an additive effect of decreased alertness. Similarly, chlorpromazine in combination with zolpidem produced no pharmacokinetic interaction, but there was an additive effect of decreased alertness and psychomotor performance.
A study involving haloperidol and zolpidem revealed no effect of haloperidol on the pharmacokinetics or pharmacodynamics of zolpidem. The lack of a drug interaction following single-dose administration does not predict the absence of an effect following chronic administration.
An additive adverse effect on psychomotor performance between alcohol and oral zolpidem was demonstrated [see Warnings and Precautions (5.1)].
Following five consecutive nightly doses at bedtime of oral zolpidem tartrate 10 mg in the presence of sertraline 50 mg (17 consecutive daily doses, at 7:00 am, in healthy female volunteers), zolpidem Cmax was significantly higher (43%) and Tmax was significantly decreased (-53%). Pharmacokinetics of sertraline and N-desmethylsertraline were unaffected by zolpidem.
A single-dose interaction study with zolpidem tartrate 10 mg and fluoxetine 20 mg at steady-state levels in male volunteers did not demonstrate any clinically significant pharmacokinetic or pharmacodynamic interactions. When multiple doses of zolpidem and fluoxetine were given at steady state and the concentrations evaluated in healthy females, an increase in the zolpidem half-life (17%) was observed. There was no evidence of an additive effect in psychomotor performance.
Drugs that Affect Drug Metabolism via Cytochrome P450
Some compounds known to inhibit CYP3A may increase exposure to zolpidem. The effect of inhibitors of other P450 enzymes on the pharmacokinetics of zolpidem is unknown.
A single-dose interaction study with zolpidem tartrate 10 mg and itraconazole 200 mg at steady-state levels in male volunteers resulted in a 34% increase in AUC0-∞ of zolpidem tartrate. There were no pharmacodynamic effects of zolpidem detected on subjective drowsiness, postural sway, or psychomotor performance.
A single-dose interaction study with zolpidem tartrate 10 mg and rifampin 600 mg at steady-state levels in female subjects showed significant reductions of the AUC (-73%), Cmax (-58%), and T1/2 (-36 %) of zolpidem together with significant reductions in the pharmacodynamic effects of zolpidem tartrate. Rifampin, a CYP3A4 inducer, significantly reduced the exposure to and the pharmacodynamic effects of zolpidem.
A single-dose interaction study with zolpidem tartrate 5 mg and ketoconazole, a potent CYP3A4 inhibitor, given as 200 mg twice daily for 2 days increased Cmax of zolpidem (30%) and the total AUC of zolpidem (70%) compared to zolpidem alone and prolonged the elimination half-life (30%) along with an increase in the pharmacodynamic effects of zolpidem. Consideration should be given to using a lower dose of zolpidem when ketoconazole and zolpidem are given together.
Other Drugs with No Interactions with Zolpidem
A study involving cimetidine/zolpidem tartrate and ranitidine/zolpidem tartrate combinations revealed no effect of either drug on the pharmacokinetics or pharmacodynamics of zolpidem.
Zolpidem tartrate had no effect on digoxin pharmacokinetics and did not affect prothrombin time when given with warfarin in healthy subjects.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis: Zolpidem was administered in the diet to rats and mice for 2 years at doses of 4, 18, and 80 mg base/kg/day. In mice, these doses are approximately 7, 30, and 140 times, respectively, the recommended human dose (RHD) of 3.5 mg/day (approximately 2.8 mg zolpidem base) on a mg/m2 basis. In rats, these doses are approximately 15, 60, and 280 times, respectively, the RHD on a mg/m2 basis. No evidence of carcinogenic potential was observed in mice. In rats, renal tumors (lipoma, liposarcoma) were seen at the mid- and high doses.
Mutagenesis: Zolpidem was negative in in vitro (bacterial reverse mutation, mouse lymphoma, and chromosomal aberration) and in vivo (mouse micronucleus) genetic toxicology assays.
Impairment of fertility: Oral administration of zolpidem (doses of 4, 20, and 100 mg base/kg/day) to rats prior to and during mating, and continuing in females through postpartum day 25, resulted in irregular estrus cycles and prolonged precoital intervals at the highest dose tested. The no-effect dose for these findings is approximately 70 times the RHD on a mg/m2 basis. There was no impairment of fertility at any dose tested.
14 CLINICAL STUDIES
14.1 Middle-of-the-Night Awakening Trials
Intermezzo was evaluated in two randomized, double-blind, placebo-controlled studies (Studies 1 and 2) in patients with insomnia characterized by difficulty returning to sleep after a middle-of-the-night (MOTN) awakening. In these studies, patients met the diagnosis for primary insomnia as defined by the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR) and had at least three prolonged MOTN awakenings per week that were at least 30 minutes in duration.
Sleep Laboratory Study (Scheduled Dosing)
Adult patients aged 19 to 64 years (N=82; 58 female, 24 male) with a history of difficulty returning to sleep after middle-of-the-night awakenings were evaluated in a double-blind, placebo-controlled, 3-period cross-over sleep laboratory study (Study 1). The primary outcome measure was latency to persistent sleep (LPS).
Doses of 3.5 mg and 1.75 mg of Intermezzo significantly decreased both objective (by polysomnography) and subjective (patient-estimated) sleep latency after a scheduled middle-of-the-night awakening as compared to placebo. The effect on sleep latency was similar for females receiving 1.75 mg of Intermezzo and males receiving 3.5 mg of Intermezzo.
Outpatient Study (As-needed Dosing)
Adult patients aged 18 to 64 years (N=295; 201 women, 94 men) with difficulty returning to sleep after middle-of-the-night awakenings were evaluated in a double-blind, placebo-controlled 4-week outpatient study of Intermezzo. Patients took study drug (3.5 mg of Intermezzo or placebo) on an as-needed (prn) basis, when they had difficulty returning to sleep after waking in the middle of the night, provided they had at least 4 hours time remaining in bed. Subjective (patient-estimated) time to fall back to sleep after middle-of-the-night awakening was significantly shorter for Intermezzo 3.5 mg compared to placebo.
14.2 Special Safety Studies
Driving Study
A randomized, double-blind, placebo-controlled, active-control, single-center, four-period, crossover study in 40 healthy subjects was conducted to evaluate the effects of middle-of-the-night administration of Intermezzo on next-morning driving performance. The four randomized treatments included Intermezzo 3.5 mg four hours before driving, Intermezzo 3.5 mg three hours before driving, placebo, and a positive control (an unapproved sedative-hypnotic) given nine hours before driving.
The primary outcome measure was the change in the standard deviation of lateral position (SDLP), a measure of driving impairment. The results were analyzed using a symmetry analysis, which determined the proportion of subjects whose change from their own SDLP in the placebo condition was statistically significantly above a threshold thought to reflect clinically meaningful driving impairment.
When driving began 3 hours after taking Intermezzo, testing had to be terminated for one subject (a 23-year old woman) due to somnolence. Overall, the symmetry analysis showed a statistically significant impairing effect at 3 hours. When driving began 4 hours after taking Intermezzo, statistically significant impairment was not found, but numerically Intermezzo was worse than placebo. Zolpidem blood levels were not measured in the driving study, and the study was not designed to correlate specific blood level with degree of impairment. However, the estimated blood level of zolpidem in patients whose SDLP worsened according to the symmetry analysis is considered to present a risk for driving impairment. In some women, the 3.5 mg dose of Intermezzo results in zolpidem blood levels that remain at or sometimes considerably above this level 4 or more hours after dosing. Therefore, the recommended dose for women is 1.75 mg. A small negative effect on SDLP may remain in some patients 4 hours after the 1.75 mg dose in women, and after the 3.5 mg dose in men, such that a potential negative effect on driving cannot be completely excluded.
Rebound effects
In studies performed with other zolpidem formulations (5 mg to 10 mg oral zolpidem tartrate) given at bedtime, there was no objective (polysomnographic) evidence of rebound insomnia at recommended doses seen in studies evaluating sleep on the nights following discontinuation. There was subjective evidence of impaired sleep in the elderly on the first post-treatment night at doses above the recommended elderly dose of 5 mg oral zolpidem tartrate.
Memory impairment in controlled studies
Controlled studies in adults utilizing objective measures of memory yielded no consistent evidence of next-day memory impairment following the administration at bedtime of 5 mg to 10 mg oral zolpidem tartrate. However, in one study involving zolpidem tartrate doses of 10 mg and 20 mg, there was a significant decrease in next-morning recall of information presented to subjects during peak drug effect (90 minutes post-dose), i.e., these subjects experienced anterograde amnesia. There was also subjective evidence from adverse event data for anterograde amnesia occurring in association with the administration of oral zolpidem tartrate, predominantly at doses above 10 mg.
16 HOW SUPPLIED/STORAGE AND HANDLING
Each sublingual tablet is individually packaged in a unit-dose pouch.
Intermezzo 1.75 mg tablets are yellow, round, uncoated, biconvex, debossed with ZZ on one side and supplied as:
NDC 59011-256-30: Carton of 30 unit-dose pouches
Intermezzo 3.5 mg tablets are beige, round, uncoated, biconvex, debossed with ZZ on one side and supplied as:
NDC 59011-255-30: Carton of 30 unit-dose pouches
Storage and Handling
Store between 20°C to 25°C (68°F to 77°F). Excursions permitted between 15°C and 30°C (59°F and 86°F). Protect from moisture.
The patient should be instructed not to remove the sublingual tablet from the unit-dose pouch until the patient is ready to consume it.
17 PATIENT COUNSELING INFORMATION
See FDA-approved patient labeling (Medication Guide).
Inform patients and their families about the benefits and risks of treatment with Intermezzo. Inform patients of the availability of a Medication Guide and instruct them to read the Medication Guide prior to initiating treatment with Intermezzo and with each prescription refill. Review the Intermezzo Medication Guide with every patient prior to initiation of treatment. Instruct patients or caregivers that Intermezzo should be taken only as prescribed.
CNS depressant Effects and Next-Day Impairment
Tell patients that Intermezzo has the potential to cause next-day impairment, and that this risk is increased if dosing instructions are not carefully followed. Tell patients to wait for at least 4 hours after dosing and until they feel fully awake before driving or engaging in other activities requiring full mental alertness.
Severe Anaphylactic and Anaphylactoid Reactions
Inform patients that severe anaphylactic and anaphylactoid reactions have occurred with zolpidem. Describe the signs/symptoms of these reactions and advise patients to seek medical attention immediately if any of them occur.
Sleep-driving and Other Complex Behaviors
Instruct patients to inform their families that zolpidem has been associated with “sleep-driving” and other complex behaviors while not being fully awake (preparing and eating food, making phone calls, or having sex), and tell patients and their families to call their healthcare providers immediately if they develop any of these symptoms.
Suicide
Tell patients to immediately report any suicidal thoughts.
Administration Instructions
For detailed instructions on how to use Intermezzo, tell patients to refer to the Patient Instructions for Use.
Tell patients that Intermezzo is to be taken only once per night if needed if they wake in the middle of the night and have difficulty returning to sleep. Tell patients that Intermezzo should only be taken if they have 4 hours of bedtime remaining before the planned time of waking.
Instruct the patient to place the tablet under the tongue, allowing it to disintegrate completely before swallowing. Tell the patient that Intermezzo should not be swallowed whole.
Tell patients that the effect of Intermezzo may be slowed if taken with or immediately after a meal.
Instruct patients to remove the tablet from the unit-dose pouch just prior to dosing.
Advise patients NOT to take Intermezzo if they drank alcohol that day or before bed.
Healthcare professionals can telephone Purdue Pharma’s Medical Services Department (1-888-726-7535) for information on this product.
Distributed by:
Purdue Pharma L.P.,
Stamford, CT 06901-3431
Manufactured by: Patheon Pharmaceuticals, Inc., Cincinnati, OH 45237
U.S. Patent Numbers 7658945; 7682628; 8,242,131; 8,252,809
©2015, Purdue Pharma L.P.
MEDICATION GUIDE
Intermezzo® (in ter mét zoh)
(zolpidem tartrate) sublingual tablet CIV
Read the Medication Guide that comes with Intermezzo® before you start taking it and each time you get a refill. There may be new information. This Medication Guide does not take the place of talking to your doctor about your medical condition or treatment.
What is the most important information I should know about Intermezzo?
Follow the Instructions for Use at the end of this Medication Guide when you take Intermezzo. If you do not follow the Instructions for Use, you might be drowsy in the morning without knowing it.
- Only take one tablet a night, if needed.
- Only take Intermezzo if you have at least 4 hours of bedtime left.
Intermezzo may cause serious side effects, including:
- After taking Intermezzo, you may get up out of bed while not being fully awake and do an activity that you do not know you are doing. The next morning, you may not remember that you did anything during the night. You have a higher chance for doing these activities if you drank alcohol that day or take other medicines that make you sleepy with Intermezzo. Reported activities include:
- driving a car ("sleep-driving")
- making and eating food
- talking on the phone
- having sex
- sleep-walking
Call your healthcare provider right away if you find out that you have done any of the above activities after taking Intermezzo.
Important:
- Take Intermezzo exactly as prescribed
- Do not take Intermezzo if you:
- drank alcohol that day or before bed.
- took another medicine to help you sleep.
- do not have at least 4 hours of bedtime remaining.
What is Intermezzo?
Intermezzo is a sedative-hypnotic (sleep) medicine. Intermezzo is used in adults for the treatment of a sleep problem called insomnia. Many people have difficulty returning to sleep after awakening in the middle of the night. Intermezzo is designed to specifically treat this problem.
It is not known if Intermezzo is safe and effective in children.
Intermezzo is a federally controlled substance (CIV) because it can be abused or lead to dependence. Keep Intermezzo in a safe place to prevent misuse and abuse. Selling or giving away Intermezzo may harm others, and is against the law. Tell your doctor if you have ever abused or have been dependent on alcohol, prescription medicines, or street drugs.
Who should not take Intermezzo?
- Do not take Intermezzo if you are allergic to zolpidem or any other ingredients in Intermezzo. See the end of this Medication Guide for a complete list of ingredients in Intermezzo.
- Do not take Intermezzo if you have had an allergic reaction to drugs containing zolpidem, such as Ambien, Ambien CR, Edluar, or Zolpimist.
Symptoms of a serious allergic reaction to Intermezzo can include:
- swelling of your face, lips, and throat that may cause difficulty breathing or swallowing
- nausea and vomiting
Intermezzo may not be right for you. Before starting Intermezzo, tell your doctor about all of your health conditions, including if you:
- have a history of depression, mental illness, or suicidal thoughts
- have a history of drug or alcohol abuse or addiction
- have kidney or liver disease
- have a lung disease or breathing problems
- are pregnant, planning to become pregnant, or breastfeeding
Tell your doctor about all of the medicines you take, including prescription and nonprescription medicines, vitamins, and herbal supplements. Medicines can interact with each other, sometimes causing serious side effects. Your doctor will tell you if you can take Intermezzo with your other medicines.
Know the medicines you take. Keep a list of your medicines with you to show your doctor and pharmacist each time you get a new medicine.
How should I take Intermezzo?
- See “What is the most important information I should know about Intermezzo”
- Read the "Instructions for Use" at the end of this Medication Guide for detailed instructions on how to take Intermezzo.
- Take Intermezzo exactly as prescribed. Only take one Intermezzo tablet per night if needed.
- Do not take Intermezzo if you drank alcohol that evening or before bed.
- While in bed, place the tablet under your tongue and allow it to break apart completely. Do not swallow it whole.
- You should not take Intermezzo with or right after a meal. Intermezzo may help you fall asleep faster when you take it on an empty stomach.
- Call your health care provider if your insomnia worsens or is not better within 7 to 10 days. This may mean that there is another condition causing your sleep problem.
- If you take too much Intermezzo or overdose, get emergency treatment.
What are the possible side effects of Intermezzo?
Intermezzo may cause serious side effects, including:
- getting out of bed while not being fully awake and doing an activity that you do not know you are doing. (See “What is the most important information I should know about Intermezzo?”)
- abnormal thoughts and behavior. Symptoms include more outgoing or aggressive behavior than normal, confusion, agitation, hallucinations, worsening of depression, and suicidal thoughts or actions.
- memory loss
- anxiety
- severe allergic reactions. Symptoms include swelling of the tongue or throat, trouble breathing, and nausea and vomiting. Get emergency medical help if you get these symptoms after taking Intermezzo.
Call your health care provider right away if you have any of the above side effects or any other side effects that worry you while using Intermezzo.
The most common side effects of Intermezzo are:
Even if you follow the Instructions for Use, you may still feel drowsy in the morning after taking Intermezzo. Do not drive or do other dangerous activities after taking Intermezzo until you are fully awake.
These are not all the side effects of Intermezzo. Ask your health care provider or pharmacist for more information.
You may report side effects to FDA at 1-800-FDA-1088.
How should I store Intermezzo?
- Store Intermezzo at room temperature, 68° to 77°F (20° to 25°C). Protect from moisture.
- Only open the pouch when you are ready to use Intermezzo.
Keep Intermezzo and all medicines out of reach of children.
General Information about Intermezzo
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use Intermezzo for a condition for which it was not prescribed. Do not give Intermezzo to other people, even if you think they have the same symptoms that you have. It may harm them and it is against the law.
This Medication Guide summarizes the most important information about Intermezzo. If you would like more information, talk with your doctor. You can ask your doctor or pharmacist for information about Intermezzo that is written for healthcare professionals. For more information about Intermezzo, call Purdue Pharma at 1-888-726-7535 or go to www.purduepharma.com or www.intermezzorx.com.
What are the ingredients in Intermezzo?
Active Ingredient: Zolpidem tartrate
Inactive Ingredients: Each Intermezzo tablet includes the following inactive ingredients: mannitol, sorbitol, crospovidone, silicon dioxide, sodium carbonate, sodium bicarbonate, croscarmellose sodium, sodium stearyl fumarate, silicon dioxide, natural and artificial spearmint flavor, silicon dioxide-colloidal, and sucralose. The 1.75 mg tablet also contains yellow iron oxide, and the 3.5 mg tablet contains beige iron oxide.
Rx only
This Medication Guide has been approved by the U.S. Food and Drug Administration.
Distributed by:
Purdue Pharma L.P.
Stamford, CT 06901-3431
Issued: February 2013
Instructions for Use
Intermezzo® (in ter mét zoh)
(zolpidem tartrate) sublingual tablet CIV
Read these Instructions for Use before you start taking Intermezzo and each time you get a refill. There may be new information. This information does not take the place of talking to your healthcare provider about your medical condition or your treatment.
What is the most important Information I should know about Intermezzo?
Follow these Instructions for Use when you take Intermezzo. If you do not follow these instructions, you might be drowsy in the morning without knowing it.
- Only take 1 tablet a night if needed
- Only take Intermezzo if you have at least 4 hours of bedtime left
Using Intermezzo the wrong way can make you drowsy in the morning.
Before you go to bed:
- Place only 1 Intermezzo pouch by your bed, and have a clock or watch nearby (see Figure A).
Figure A - Store all other unopened Intermezzo pouches with your other medicines away from your bedside.
- Only open the Intermezzo pouch when you are ready to use it.
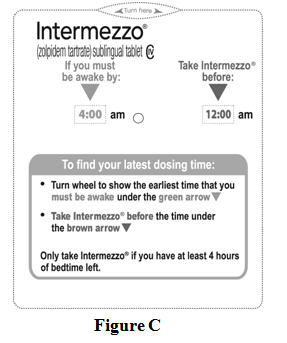
- You can either use the Intermezzo Dosing Time Chart (see Figure B) or the Dosing Time Tool (see Figure C) that comes with Intermezzo to find the latest time during the night you can take Intermezzo.
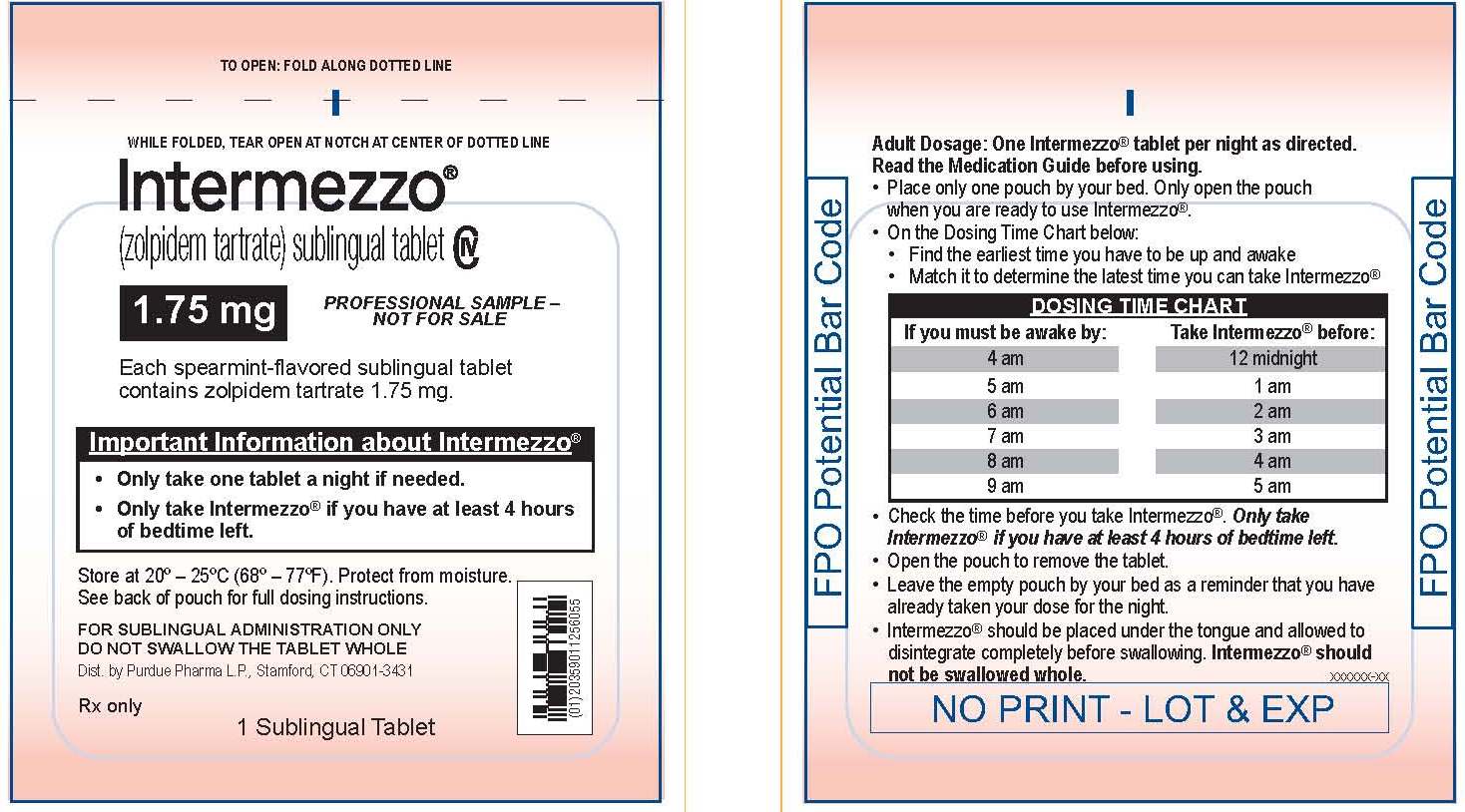
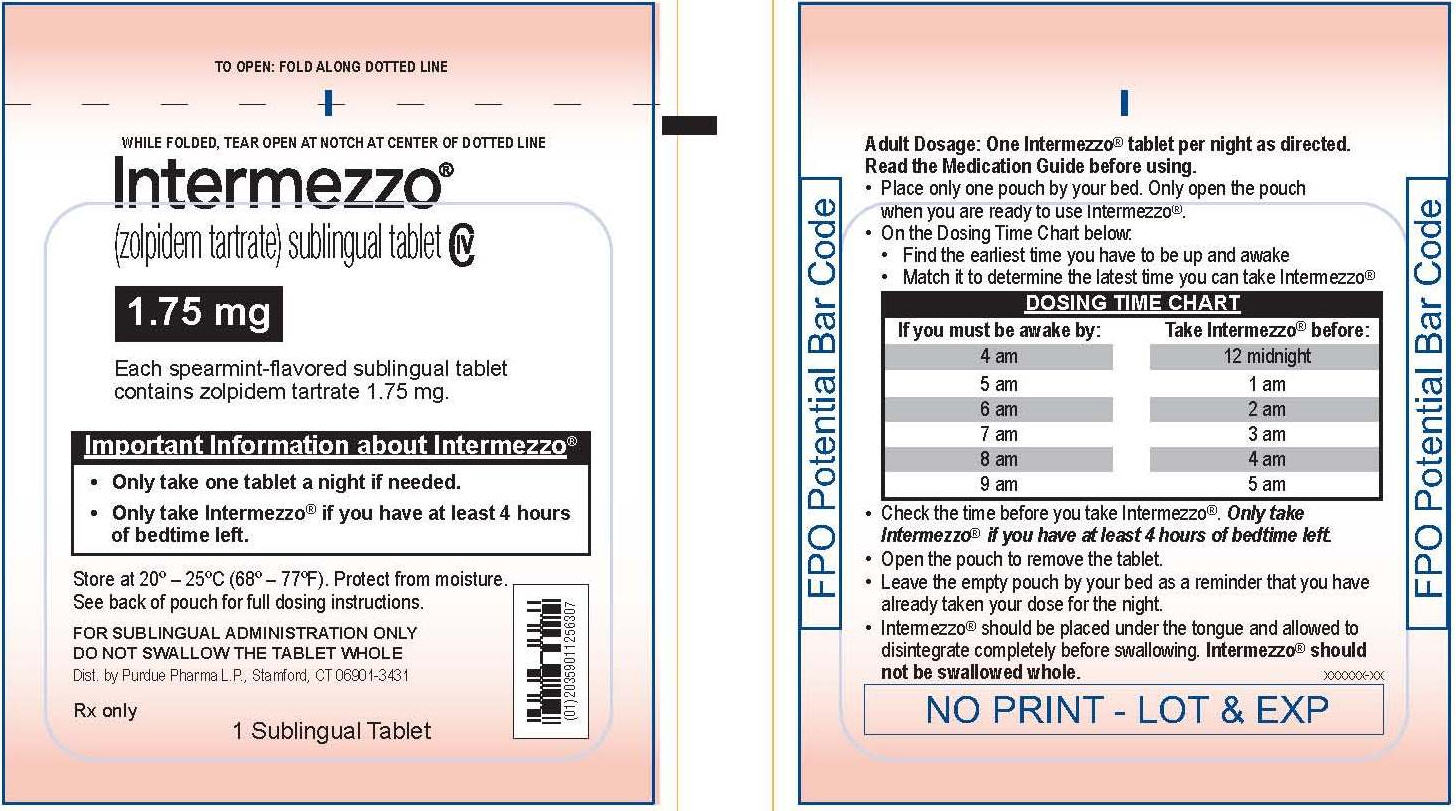
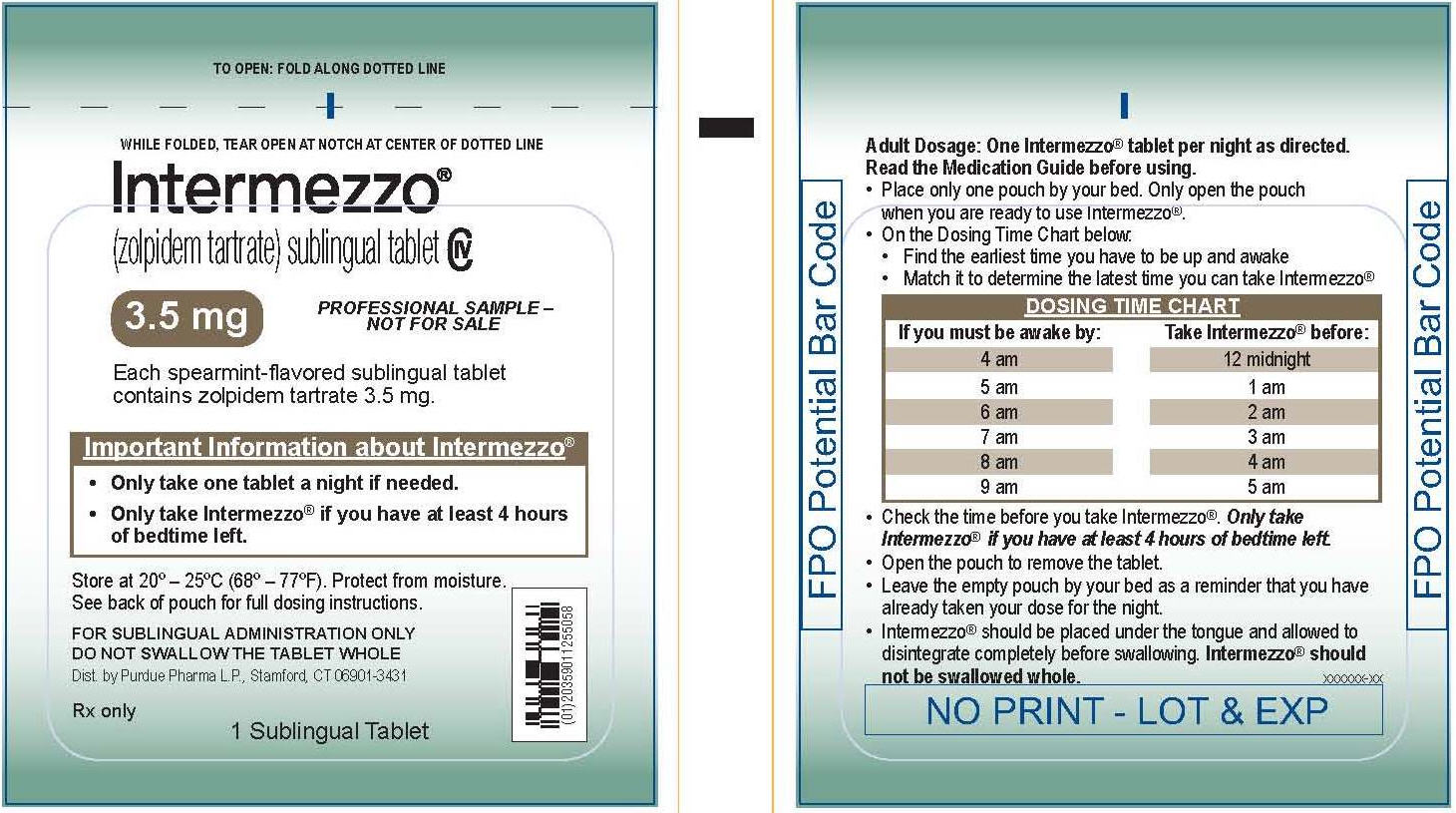
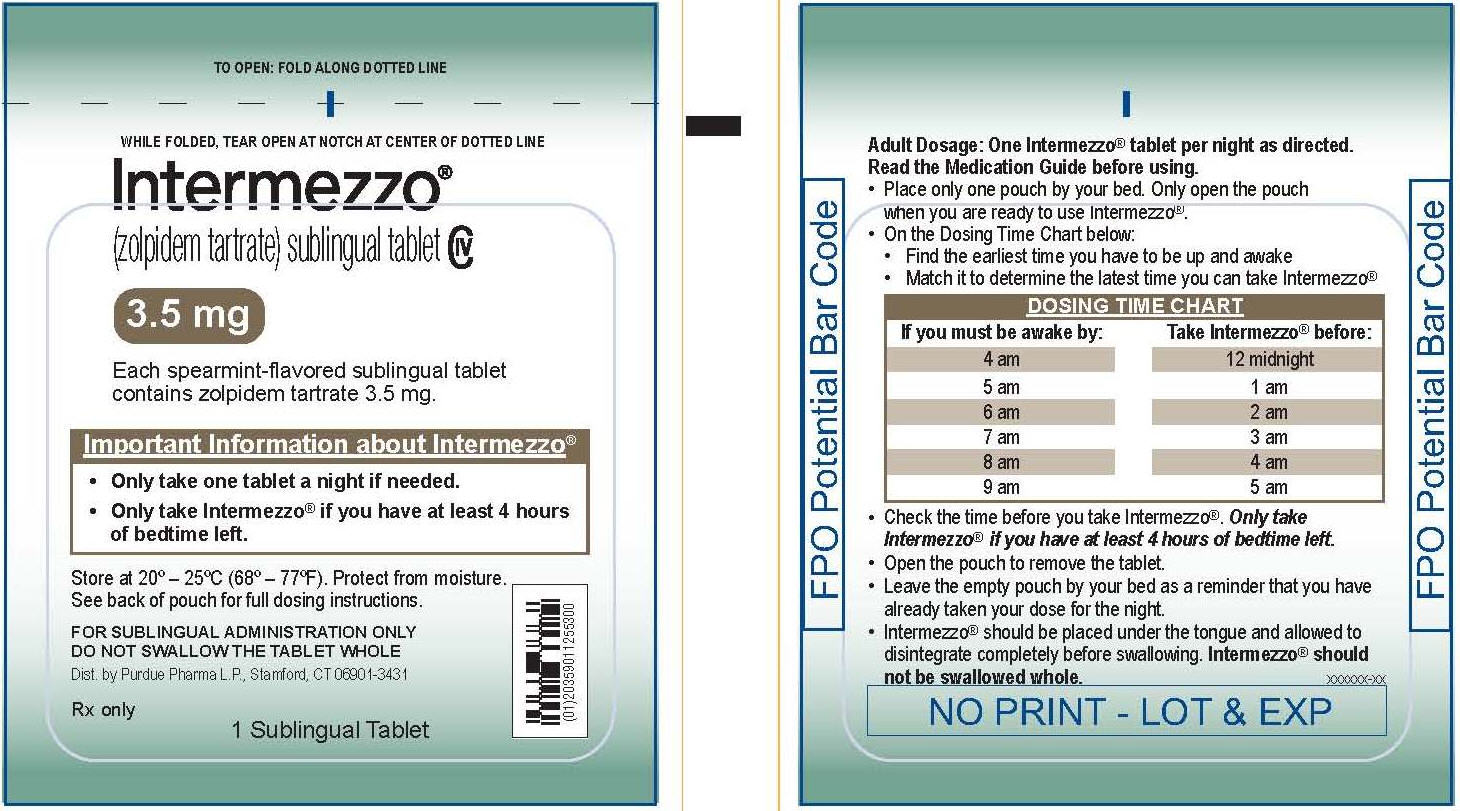
Intermezzo Dosing Time Chart (see Figure B):
- You can take Intermezzo if you have at least 4 hours of bedtime left before you must be awake.
- Find the earliest time you have to be up and awake in the column on the left.
- Find the latest time you can take Intermezzo on the same line in the column on the right.
Intermezzo Dosing Time Chart| Figure B |
If you must
be awake by: | Take
Intermezzo before: |
| 4 am | 12 midnight |
| 5 am | 1 am |
| 6 am | 2 am |
| 7 am | 3 am |
| 8 am | 4 am |
| 9 am | 5 am |
Intermezzo Dosing Time Tool (see Figure C):
- Turn the Intermezzo Dosing Time Tool wheel to show the earliest time that you must be awake under the green arrow.
- Take Intermezzo before the time under the brown arrow.
During the night when you take Intermezzo:
Step 1. Check the current time and use the Intermezzo Dosing Time Chart or the Intermezzo Dosing Time Tool to decide if you should take Intermezzo.
- Only take Intermezzo if you have at least 4 hours of bedtime left before you have to be awake (see Figure B).
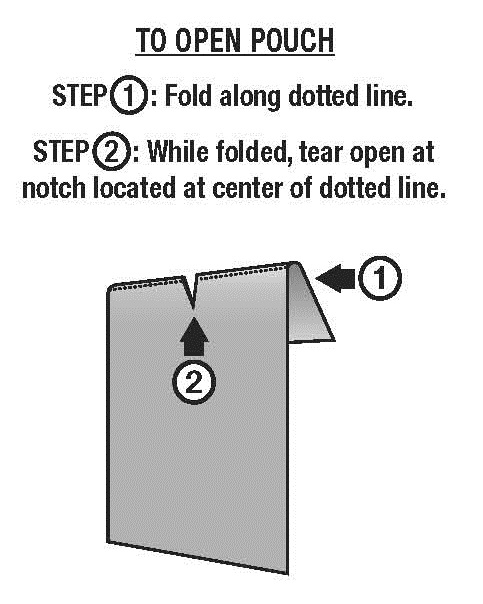
Step 2. Open the Intermezzo pouch you placed by your bed.
- Fold the Intermezzo pouch along the dotted line. While the Intermezzo pouch is folded, tear the pouch open at the notch at the center of the dotted line (see Figure D).
Step 3. Remove the tablet from the Intermezzo pouch.
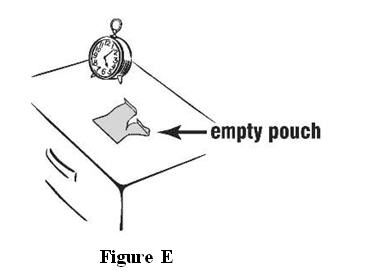
Step 4. Leave the empty Intermezzo pouch where you can see it. The empty pouch will help remind you that you already took your Intermezzo dose (see Figure E).
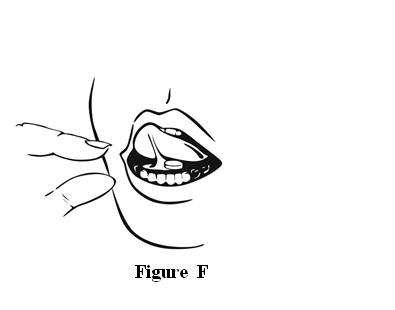
Step 5. While in bed, place the Intermezzo tablet under your tongue and allow it to break apart completely, then swallow. Do not swallow it whole (see Figure F).
Step 6. Throw the empty Intermezzo pouch away in the morning.
When you wake up in the morning, be sure that at least 4 hours have passed since you have taken Intermezzo and you feel fully awake before driving. Do not do dangerous activities until you know how Intermezzo affects you.
This Medication Guide and Instructions for Use have been approved by the U.S. Food and Drug Administration.
Distributed by:
Purdue Pharma L.P.
Stamford, CT 06901-3431
Issued: February 2013
INTERMEZZO (zolpidem tartrate) sublingual tablets
NDC:59011-256
Pouch
INTERMEZZO (zolpidem tartrate) sublingual tablets
NDC:59011-256
Carton
INTERMEZZO (zolpidem tartrate) sublingual tablets
NDC:59011-255
Pouch
INTERMEZZO (zolpidem tartrate) sublingual tablets
NDC:59011-255
Carton
INTERMEZZO
zolpidem tartrate tablet |
|
|
|
|
|
INTERMEZZO
zolpidem tartrate tablet |
|
|
|
|
|
Revised: 07/2015 Purdue Pharma LP